Evidence on the evaluation of the impact of strategies implemented in these countries for obesity prevention
In general, our literature review evidenced a lack of reports and studies evaluating the strategies mentioned in the previous section. Nosotros study here the studies/reports plant by strategy.
At the level of obesity strategic plans, in 2014, all countries in Latin America signed the Program of Activeness for the Prevention of Obesity in Children and Adolescents(vi,viii) . This plan adopts a preventive, multi-sectorial and life-class arroyo and considers the social determinants of health. Information technology aims at promoting an environment that is conducive to healthy eating and a higher concrete activity level and making the healthier option the easier option. To support countries in the fight against obesity, PAHO provides technical guidelines and cooperation, advocates for programmes and policies and fosters collaboration amid countries. Besides PAHO has other documents to assist member states in this endeavour(9). Also, the Council of Ministries of Health in Cardinal America developed the Plan for the Prevention of Obesity in Children and Adolescents in 2014–2025(ten). In 2015, a meeting in Panama with experts from Healthy Latin America Coalition, PAHO/WHO, the Ministry of Health of Panama, and others discussed the need for a stronger part of the civil society in supporting and promoting policies on food, tobacco, booze and level of concrete activity in the region(eleven). In 2016, the Caribbean Public Wellness Agency and PAHO in collaboration with the Ministries of Health from countries with successful obesity prevention policies, such equally Mexico and Republic of chile, adult a roadmap to forestall childhood obesity(12). This is of import as lessons learned from efforts that have or accept not worked in different countries should be shared. In addition, multi-national studies tin provide rich information and insights into how unlike strategies work with different cultures, ethnic backgrounds, environments, etc. Too, the Non-Catching Diseases Alliance developed a Civil Club Action Program for 2017–2021 on Preventing Childhood Obesity in the Caribbean area(thirteen). Lastly, several institutions accept convened experts from PAHO, FAO and the National Institutes of Wellness's Fogarty International Middle(Reference Caballero, Vorkoper and Anandfourteen) to evaluate the situation.
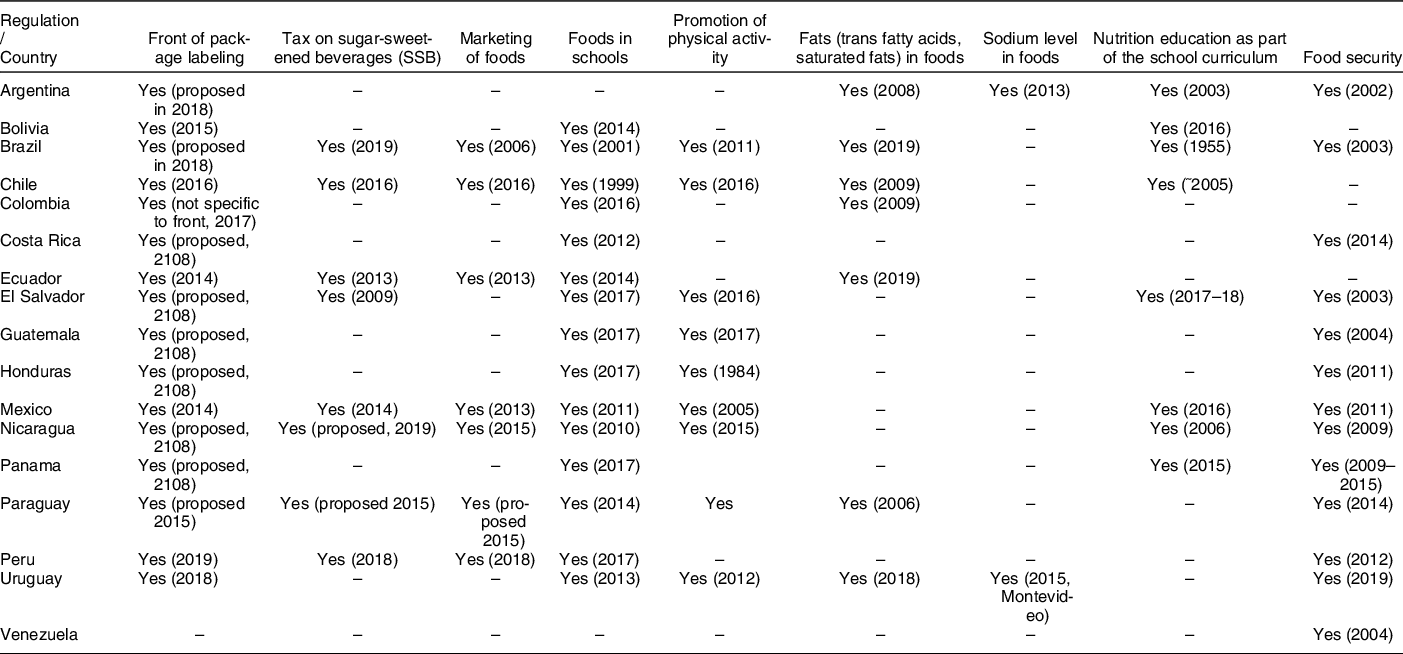
At the level of nutritional policies, there are a few successful strategies in terms of acceptance, reach or effectiveness in changing behaviours in Latin America that should be discussed:
Front-of-packet label: At the Coming together of Ministers of Health of Central America in 2017, a proposed resolution to plant a front-of-packet organization for nutritional warnings was endorsed(15). Also, in 2018, the Ministers of Health of MERCOSUR (the Southern Common Market) agreed on a set up of principles to promote compulsory front-of-package labelling systems to indicate excessive sugar, Na and/or fat content(xvi). A study evaluating different labels pattern for front-of-package labels in m participants from all twelve countries participants of MERCOSUR in 2018 found that the modify in labelling significantly improved the power of individuals to rank products according to their nutritional quality(Reference Egnell, Talati and Hercberg17). As well, a study in Republic of chile done 6 months afterward the implementation of this regulation plant that 67 % of participants selected products with fewer warnings in the label and that the presence of 'high in' stamps influenced the purchase decision amongst 90 %(xviii). Also, information technology has been estimated that nutrient companies have modified one of every 5 products to make it healthier (2015–2016)(Reference Boza, Guerrero and Barreda19). In Ecuador, a study conducted a 1-twelvemonth mail service-implementation of this strategy (2015) found that it was widely recognised and understood(Reference Díaz, Veliz and Rivas-Mariño20). In two supermarkets in Quito among seventy-three participants, 88 % reported knowing about this arrangement and 28 % used it, which showed that it significantly influenced their shopping(Reference Teran, Hernandez and Freire21). In Mexico, a survey among parents of children in uncomplicated schools found that 51 % used the displayed nutrient content and reported to adopt the new traffic light system compared with the traditional organization(22). In Uruguay, a study found that 95 % of respondents saw the front of package labelling police as positive, regardless of age, gender or socio-economic status(Reference Ares, Aschemann-Witzel and Curutchet23). A greater percentage of individuals from low socio-economical groups (xc %) said the characterization would help them improve the quality of their diets, compared with those with a medium (86 %) and loftier (84 %) socio-economic status(Reference Ares, Aschemann-Witzel and Curutchet23). The bear witness on the effectiveness of this strategy is considered medium equally at that place is limited testify from studies in different countries and most have non included a representative sample of the population.
Saccharide-sweetened beverages taxation: A recent review focused merely on Latin American countries found that at to the lowest degree thirty-nine sugar-sweetened beverage regulatory initiatives have been adapted(Reference Bergallo, Castagnari and Fernández24). From these, twenty-eight regulatory initiatives were passed by legislative and executive bodies and 11 are self-regulatory initiatives by the beverage industries. Also, 86 % of regulations past the government are binding; 56 % describe how to monitor and evaluate this, 62 % call for specific sanctions and 20 three specify who the body in accuse of this monitoring. In Chile, a sugar-sweetened beverage with more than 6·25 g of carbohydrate per 100 ml is taxed at xviii %, while carbohydrate-sweetened beverage below this threshold is taxed at 10 %. In Ecuador, a revenue enhancement of USD 0·xviii/100 grand sugar on carbohydrate-sweetened beverages with more than than 25 g of carbohydrate per liter. In Mexico, the revenue enhancement is 1 peso (which is well-nigh 0·05 USD) per liter and also an viii % taxation on snacks with more than than 275 kcal per 100 one thousand. In Peru, a tax of 50 % is imposed on beverages with more than 6 m per 100 ml. In Brazil, El Salvador and Nicaragua, this is at the proposal phase. In Colombia and Argentina, the strong industry lobbying impeded its implementation. The experience of Mexico and Chile is the virtually studied so far, as this was implemented a few years ago (2014 in Mexico and 2016 in Chile). In Chile, the results showed that there was a highly significant 22 % subtract in the monthly purchased volume of the higher-taxed, sugary soft drinks(Reference Nakamura, Mirelman and Cuadrado25). The reduction in soft drink purchasing was about evident amidst higher socio-economical groups and higher pretax purchasers of sugary soft drinks. In Mexico, taxed beverages purchases decreased from 200 ml/d at the finish of 2013 (just earlier the implementation of the beverage taxation) to about 160 mg/d at the end of 2014 (after virtually 1 yr of the tax implementation), which represents a refuse of 12 %(Reference Colchero, Rivera-Dommarco and Popkin26,Reference Colchero, Popkin and Rivera27) . Reductions were higher among the households of low socioeconomic condition (17 % decrease by the terminate of 2014 compared with pretax trends). Also, purchases of untaxed beverages were 4 % (36 ml/capita/d) higher, mainly driven by water. The evidence on the effectiveness of this strategy is considered medium as in that location is limited evidence from studies in different countries and virtually have not included a representative sample of the population.
Regulation for the marketing of foods: These initiatives have varied widely by country, with some having formulated guidance, while other restrictions, with some sanctions, merely most practice not have a articulate clarification of their monitoring. Banning unhealthy food ad may have a positive impact on children's diets. A review in Brazil showed that most studies were based on constabulary analysis or qualitative written report of advertisement, and several companies had differences in ethical behaviour regarding food advertisements, showing a lack of delivery to the policies on food advertisements(Reference Kassahara and Sarti28). Then far, Chile is the country that has implemented the nearly comprehensive regulation of food publicity, regulating 35–45 % of candy foods and beverages high in added carbohydrate, Na or saturated fat. Also, there is a ban on the marketing of certain unhealthy foods during selected child Idiot box programmes. In United mexican states, the regulation prohibits advertising of unhealthy foods and beverages to children mainly in TV or flick theatres, with some exceptions for sure programmes. Brazil limits all publicity targeting nutrient for children. Republic of bolivia, Chile and Mexico also require to include messages to promote healthy lifestyles, and Brazil, Chile, Republic of ecuador, Mexico and Peru require the inclusion of warning messages most the potential health effects of sure products(Reference Bergallo, Castagnari and Fernández24). Republic of ecuador and Nicaragua are at the proposal phase to implement it, while in Argentina, it was vetoed by the President(Reference Bergallo, Castagnari and Fernández24). In Mexico, an analysis of children'south advertisements in 2012–2013 in the nearly pop public TV showed that about 75 % of the total food and beverage advertisements were aimed directly or indirectly at children(Reference Théodore, Tolentino-Mayo and Hernández-Zenil29). Even amidst companies that had signed the cocky-regulation, more than than 31 % of the advertising of unhealthy products were aimed at children or adolescents. A review of twenty-3 studies (six in Chile, 5 in Mexico, four in Brazil, three amongst Hispanics in the The states and one in Argentina, Republic of peru, Republic of colombia, Honduras and Venezuela) about food advertising directed to children on TV found a loftier exposure of TV food advertised for children and their family, which has been associated with preference and buy of unhealthy foods and with overweight and obesity(Reference Bacardí-Gascón and Jiménez-Cruz30). The evidence on the effectiveness of this strategy is also considered medium.
School repast programmes: But a few studies are evaluating the effectiveness of schoolhouse-based programmes. For example, in Brazil, a study of 20-one public schools in one region in 2014 found that virtually 31 % of children were overweight, that breakfast and snacks were equanimous of 68 % of ultra-processed foods, while 92 % of the tiffin foods were unprocessed and minimally processed foods(Reference Batista, Mondini and Jaime31). In Colombia, children participating in the program may have ameliorate school performance(Reference Niny32). In Chile, this program has been shown to reduce school drop-out rates(Reference Villena33). In Mexico, the regional programme 'Wellness to Learn (Salud para Aprender)' establish a decrease in overweight and obesity from 25 % in 2010–2011 to 19 % in 2016–2017 among preschoolers, from 32 % to 30 % in uncomplicated children and from 38 % to 34 % in adolescents(Reference Trejo Hérnandez and Raya Giorguli34). They likewise establish that the % of breakfast consumption increased from 84 % in 2010–2011 to 86 % in 2016–2017, consumption of fruits and vegetables iii–iv times per week increased from 34 % to 36 % and sedentarism improved past one–two points. In Peru, the Milk Glass Programme, which impacted 61 % of children 0–6 years and 18 % of children 7–13 years, establish that 63 % of those participating had a decreased hazard of obesity(Reference Diez-Canseco and Saavedra-Garcia35). A systematic review of twenty-1 studies (n 12 092) with different types of educational interventions in children (nutritional campaigns, physical activity level and ecology changes) in Latin America institute that mixed approaches combining nutritional campaigns, physical activity level promotion and ecology changes were the about constructive interventions(Reference Mancipe Navarrete, Garcia Villamil and Correa Bautista36). The evidence on the effectiveness of this strategy is as well considered medium.
Regulation of the school environs: Irresolute the food environments can have a strong influence on the school-age population and could lead to changes in nutrient preferences and weight condition. These policies have been implemented in several countries as described previously, but they differed in their legislation and how strict they are. For example, in Brazil, Ecuador, Republic of chile, Republic of peru and Uruguay, the policies to limit saccharide-sweetened beverages in schools are through their legislative and executive, while in Costa Rica and United mexican states, this has been through executive decrees but, which may have a different touch(Reference Bergallo, Castagnari and Fernández24). Although all are mandatory, some accept not specific sanctions if schools are non in compliance, such as in Ecuador. As well, some countries are very strict in the type of beverages banned. For instance, in Peru, drinks with more than 2·5 grand of sugar per 100 ml are not allowed, while in Republic of ecuador and Uruguay, the limit is on beverages with more than seven·5 thou of saccharide per 100 ml and in Mexico near all beverages that provide calories are banned, except on Fridays(Reference Bergallo, Castagnari and Fernández24). Therefore, most legislations allow 100 % fruit juices, which can still add together to the total calories consumed per day, except for United mexican states. Also, this legislation is mostly for public schools and at the uncomplicated level. Although there are no results bachelor yet on their impact on reducing obesity, there are a few obstacles encountered in their implementation. For example, in Mexico, the food industry has shown strong opposition, which delayed the process(Reference Charvel, Cobo and Hernández-Ávila37). Also, studies in United mexican states institute that the schools lacked the space, nutrient condom measures or the structure to implement these policies(Reference Gallegos Gallegos, Barragan Lizama and Hurtado Barba38). They also lacked a strong strategy to implement this throughout and faced difficulty in irresolute culturally strong practices, among others(Reference Treviño Ronzón and Sánchez Pacheco39). The show on the effectiveness of this strategy is considered weak as there are very limited studies.
Programmes to promote physical activity: These include the modification of the school curriculum to increase concrete activity level, policies in urban planning to increase access to sidewalks and areas of recreation and concrete action, among others. A global review of the touch on of such policies on obesity found that individuals living in walkable communities, with access to parks and other recreational areas, with sports facilities or spaces for recreation in schools and greater admission to stairs, were all associated with higher levels of concrete activeness(Reference Sallis and Glanzforty). In Latin America, just a few studies are evaluating such programmes. In Republic of colombia, surveys conducted in 2009 constitute that individuals participating in the wheel route (Ciclovía) programme met the physical activity recommendation in leisure time (60 %), and most participants met it by cycling for transportation (71 %)(Reference Torres, Sarmiento and Stauber41). Another survey amongst current and former programme coordinators of lx-7 bike routes in 2014–2015 institute that the average number of participants per event was > forty 000 (forty–i 500 000) with an average length of 9·1 km (1–113·vi)(Reference Sarmiento, Díaz del Castillo and Triana42). The participation of minority populations was high (61·2 %). The electric current study also evaluated the sustainability and scaling-up of five programmes and they all met the most important factors for this, such every bit some level of government support, alliances, community appropriation, champions, organisational capacity, flexibility, perceived benefits and funding stability. All the same, at that place were several differences in their design, operations, political affiliations, funding and alliances, which may be important for the multifariousness and inclusion of different segments of the population. The evidence on the effectiveness of this strategy is considered weak as in that location are very express studies.
Efforts to reduce fatty or Na in foods: In Argentina, a law was enacted in 2013 to regulate the maximum Na levels in meat products, farinaceous foods and soups, bouillons, and dressings. If all these foods fully comply with this regulation, this would reduce Na intake by about 30 mg/d (Reference Elorriaga, Gutierrez and Romero43). In a study conducted in 2019, more than than 90 % of the nutrient products included in the national Na reduction police force in Argentina were found to be compliant(Reference Allemandi, Tiscornia and Guarnieri44). The show on the effectiveness of this strategy is besides considered weak.
Programmes to promote nutrition educational activity: In Republic of chile, the v-A-24-hour interval campaign was tested on an adult sample (northward 1897), finding later on ane year that recalls of the materials was high and that the proportion of people proverb that they consumed 3–4 servings a twenty-four hour period increased from 49 % to 51 %(Reference Vio, Albala and Kain45). Another written report in Chile found that 9 months later on the implementation of the Santiago Sano programme found that 22 % of the participants had improved their nutritional status(46). The evidence on the effectiveness of this strategy is likewise considered weak.










Comments
Post a Comment